
How we name and categorize the psychological injury of trauma is not just a clinical exercise—it quietly shapes how we understand ourselves, our experiences, and even what we believe is “valid” pain and injury. Yet trauma does not always fit neatly into tidy boxes. It can be acute or chronic, obvious or invisible, single-event or recurring, and each label highlights something different while potentially confusing something else. In trying to make sense of human suffering, we often simplify what is inherently complex. This post explores some of the distinctions along with the most common symptoms of trauma.
| This post is part of a series: stress and trauma |
Over the past several decades, there has been increasing publicly available information and social conversation about trauma. Throughout this timeframe, additional information came to the surface, often through research findings, each time further widening our understanding.
I think taking the time to sit with this type of information about the kinds of events and circumstances that pose a significant threat to safety, security, and survival, and create high risk for trauma is important. In a previous post I discussed how the prevalence of trauma is very likely more than is recognized, and more than most people realize.
Sitting with this kind of information:
- helps us have a better grasp of the likely magnitude of trauma, given the large numbers of people who experience various types of significant threat/harm.
- helps to counteract the ways we may have become desensitized to what it really means to have trauma.
- helps to legitimize the experience of trauma survivors, both those who are suffering and those who are trying to recover.
- helps us find ourselves, our experiences, and potentially our symptoms, and consider whether we might be suffering from trauma (if doing so applies to us and we’re ready).
I bet a lot of people would be able to name at least one or two different types of traumas fairly accurately. If asked, what would your answer be? There are different ways to classify or categorize trauma.
Learning about some of them can help us expand our understanding of trauma and potentially see ourselves and others differently

Categories Based on the Nature of the Significant Threat or Harm
One way to think about trauma is by categorization of the nature of the significant threat or harm. This is what most people have some sense of. The existence of significant threat or harm does not necessarily mean there will be a trauma response, as other factors are involved.
The categories are not mutually exclusive. An event or circumstance that poses a significant threat or harm can and often does fall into more than one category at the same time.
There can be a higher level of categorization:
High Threat- High Intensity Events such as natural disasters, assaults, terrorist attacks, serious car accidents. In most parts of the world these are atypical in that they do not happen to everyone regularly. They may happen a few times in a lifetime or for some fortunate people not at all. These types of events, whether trauma develops or not, leave us with a sense of feeling less safe in the world.
Interpersonal Violations occur within our most primary relationships with family members. They can include relational violations involving physical, emotional, psychological, spiritual, or social abuse or neglect, attachment/developmental violations that are specific to the child/caregiver bond during sensitive areas of development as well as family/legacy or intergenerational epigenetic changes, messages, and trauma.
Betrayals are a violation of safety and security when individuals are dependent on other individuals or institutions. They can occur in any type of interpersonal relationship, or within a community, organization, or system. Betrayals add an additional painful element to harm because trust is shattered.
Intersectional/Institutional/Systemic Violations involve unfairness, discrimination, mistreatment, disempowerment, and abuses of power and privilege related to intersectionality such as gender, race, culture, religion, sexual orientation, disability, etc. They are often embedded and layered at different levels, making them insidious.
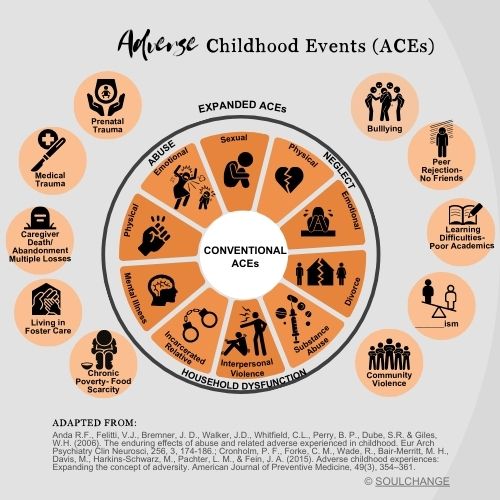
There can also be categorization by various types of Adverse Event. This approach is based on extensive research that systematically looked at adult health, functioning, and prevalence of disease, and correlated it to various adverse childhood events. The more adverse events in someone’s childhood, the more health problems and diseases in adulthood, including early death.
The original ACEs research identified 10 Adverse Childhood Events including: physical abuse, emotional abuse, and sexual abuse; physical neglect and emotional neglect; and five types of household dysfunction: mental illness; substance abuse; interpersonal violence; incarcerated relative; and parental divorce.
Additional research identified at least another 10 Adverse Childhood Events including: prenatal trauma, medical trauma, caregiver death, abandonment or multiple losses, living in foster care, chronic poverty and food scarcity, community violence, experiencing racism (and I would argue other forms of prejudice or discrimination, learning difficulties or poor academics, peer rejection or having not friends, and bullying.

Categories Based on Symptoms and Severity: PTSD versus Complex-PTSD
Another way to think about trauma is by symptoms and severity.
Trauma is a neurophysiological response whereby the brain and body physiologically, psychologically, and emotionally get stuck living/reliving the significant threat/harm that overwhelmed.
It is either considered post-traumatic stress disorder (PTSD- trauma) or complex post-traumatic stress disorder (C-PSTD- trauma).
PTSD Symptoms include:
- Intrusion symptoms associated with the traumatic event(s) such as recurrent, involuntary, and intrusive distressing memories, flashbacks and triggers.
- Avoidance symptoms of (internal and external) stimuli or reminders associated with the traumatic event(s).
- Dissociative and negative alterations in cognition and mood associated with the traumatic event(s).
- Arousal or reactivity symptoms associated with the traumatic event(s).
Complex Trauma is much more involved and results in more deeply rooted and globalized effects to the individual. Without minimizing PTSD, complex trauma has all the same symptoms as PTSD, as well a list of additional symptoms.
- Issues with coherent identity, sense of self, and/or negative self-concept. Those with complex trauma struggle with their identity, with knowing who they are, having a sense of SELF, and often will have a negative concept of themselves that is rooted in their traumatic experiences.
- Alterations in attention and consciousness. Those with complex trauma struggle not only with focus and attention, but also with staying associated or connected within themselves rather than dissociating. The reflex to dissociate was established as part of their trauma response.
- Abandonment of SELF. Some people affected by complex trauma have a pattern of abandoning themselves in various relationships and circumstances. This pattern typically develops unconsciously as an adaptation to the traumatic circumstances they survived.
- Emotion regulation difficulties and low Distress tolerance. Distress tolerance is the ability to endure difficult and stressful emotions, sensations, and circumstances, particularly when they cannot be changed or solved without making them worse or becoming overwhelmed. Those with complex trauma struggle with this and have a tendency to either avoid distress or unintentionally make matters worse, because they are easily pushed outside of their window of tolerance, they have reduced emotional intelligence, they make impulsive decisions, and can increase their own suffering by escalating the difficulty.
- Nervous system dysregulation. Those struggling with complex trauma have nervous system dysregulation. This means they tend to function, in large part, outside of their window of tolerance in survival defense states and have a hard time regulating themselves back to equilibrium and the resting state of connection and social engagement (flock).
- Lack of mind-body and mind-spirit relationship. A common result of complex trauma is disconnection with others, but also within oneself. So much energy is being used to survive and so many neurophysiological changes have taken place, including a dysregulated nervous system. This translates into gaps in mind-body and mind-spirit awareness and connection.
- Issues with attachment/insecure attachment. Impair the development of healthy, reciprocal relationships. Complex trauma is sometimes the result of traumas that occur within the child and caregiver relationship. Because the child does not receive the kind of safety, attunement, and responsiveness they need, they do not become securely attached to their caregiver, resulting in an insecure attachment style. As they grow up, this impedes their ability to develop healthy, reciprocal relationships with others.
- Learned helplessness or poor efficacy. The experiences that result in complex trauma, which among other things are defined as intolerable, overwhelming and resulting in helplessness, compromise an individual’s sense of power and efficacy. Further, living day in and day out with the symptoms of complex trauma, that can feel like heavy weight to be constantly carrying, can further reinforce the sense of learned helplessness.
- Addictions, self-harm, and other means of managing internal distress. Complex trauma involves a significant amount of internal distress from various symptoms such as a dysregulated nervous system; unprocessed emotional pain; struggles in relationships; an inability to feel safe and secure, even within oneself; living with a negative self-concept; and experiencing a lack of efficacy in one’s life. Because those struggling are not able to recognize that the distress originates inside of them because of unresolved trauma, or know how to solve these bigger issues, they seek external means to try and regulate their distress such as overworking, food, alcohol, pornography, cutting, sex, shopping, excessive exercise, etc.
- Suicidal thoughts, plans, attempts. Some individuals with complex trauma may think about or even attempt suicide as a desperate means to end the internal pain and distress they are constantly living with.
- Presence of somatic distress/somatization of Illness, chronic Illnesses, and pain conditions. E.g., migraines, GI problems, autoimmune disorders, chronic fatigue, obesity, heart disease, etc. Complex trauma results in a dysregulated nervous system that maintains heightened stress response activation, ongoing cortisol release, and changes to various neurotransmitters such as dopamine, serotonin, etc. The disrupted nervous system over a prolonged time functions like a kindling process for the development of stress related physical health issues.
In both cases, whether PTSD or Complex Trauma, there is an Underlying Neurophysiology that is present to varying degrees:
- Body and Brain physiologically, psychologically and emotionally stuck living/reliving the threat/harm.
- Brain Alterations e.g., changes to prefrontal cortex that affect attention/concentration, filtering, retaining, learning; larger amygdala; attentional bias to threat and danger; default mode network connects to past; reduced hippocampus volume.
- Dysregulated Neurotransmitters e.g., serotonin, glutamate, dopamine.
- Nervous System Dysregulation and difficulty returning to a state of homeostasis- rest & digest.
- Highly Charged Encapsulated Experiences Stored in the Brain and Body.
- Subconscious Emotional Learning Constructs.
Now What?
Hopefully, getting into some of these details about the types of trauma, including symptoms, helped you gain a better understanding of how they might be experienced.
Perhaps you were able to reframe some of the things you know about yourself or the lives of people who are important to you.
Maybe you were even able to consider other people sharing this human journey, what they might have gone through, and the types and severity of trauma they might be suffering with.
As you hold all that reflection, just notice if there is a “now what”? And if there is, consider how you might move yourself toward it in the coming days or weeks.
With Humility, Hope, and Heart,
SOURCES:
Anda R.F., Felitti, V.J., Bremner, J. D., Walker, J.D., Whitfield, C.L., Perry, B. P., Dube, S.R. & Giles, W.H. (2006). The enduring effects of abuse and related adverse experiences in childhood. Eur Arch Psychiatry Clin Neurosci, 256, 3, 174-186.
Cronholm, P. F., Forke, C. M., Wade, R., Bair-Merritt, M. H., Davis, M., Harkins-Schwarz, M., Pachter, L. M., & Fein, J. A. (2015). Adverse childhood experiences: Expanding the concept of adversity. American Journal of Preventive Medicine, 49(3), 354–361.
Larkin, H., Felitti, V., & Anda, R. (2014). Social work and adverse childhood experiences: Implications for practice and health policy. Social Work in Public Health, 29, 1-16.
Porges, S. (2019). Clinical Applications of the Polyvagal Theory: trauma, attachment, self-regulation and emotions.
Fatter, D. (2022). Trauma Treatment Certification Training Course materials.
Fisher, J. (2021). Transforming the living legacy of trauma- A Workbook for survivors and therapists.
Schwartz, A. (2024). Complex PTSD Training Course Materials.
Simington, J. (2013). Trauma Recovery Certification Course Handbook.