How trauma is understood and responded to exists on a spectrum. At one end of the continuum is a lack of understanding and responsiveness- often shaped by outdated assumptions, narrow definitions, or a lack of exposure to its broader realities. At the other end are integrated, informed, and nuanced approaches that account for complexity, context, and lived experience. Where someone sits on this continuum influences everything: how they interpret behaviour, how they respond to distress, whether certain experiences are seen at all, whether they know how to support recovery. Taking a closer look at this range helps reveal why responses to trauma can vary so widely, even within the same systems of care.
This post is part of a series: toxic stress and trauma.
Many years ago, while meeting with the Chief Operating Officer of a continuing care organization that I was working with, she talked about a new resident to one of their centres. Our meeting was about strategy and making big picture change in the organization, but I appreciated how she always started meetings with a resident story.
In a couple of sentences, she shared high-level details in terms of the woman’s age, Indigenous ancestry, diagnosis, etc. while ensuring anonymity. She talked about some of the challenges and behaviors that were occurring. She talked about unsuccessful approaches the staff had tried with the help of numerous different health disciplines, management, and a behavioral consultant.
She was not specifically asking for my thoughts. She was just sharing a story because it was puzzling her, even with her multiple decades of experience in healthcare and continuing care.
I listened quietly and then offered just one question. “Did you consider that she likely attended residential school and her being in a residential facility is bringing up all sorts of trauma?”
The staff were of course, highly trained and doing their best. I didn’t know as much as they knew in most ways. I certainly didn’t have as much frontline expertise or experience. But I did understand trauma, and so could readily see what was very likely going on. Thankfully, the organization was committed to person-centred care, so it kept looking for other approaches. It didn’t blame her, and it didn’t just medicate the reactive behaviors into submission.
Stories just like this and millions that are much, much worse, along with the last couple of decades of enlightening research about trauma have led to the development of an evolving continuum of trauma care.
Now, is that continuum of trauma care all set up? Is it available everywhere? Is it without gaps? Not even close. But it’s underway. It’s being talked about. Parts of it are being practiced in many places to the degree that makes sense for those settings.
People are pushing the envelope of our understanding. This impacts our approach and improves our response. And that’s how change happens. Change for survivors. Change for the future.
Why a Continuum of Trauma Care Matters
Let’s be honest. Continuums can feel complex. And they can even seem pretty useless until you lean in to apply them. Then, they suddenly make sense and are often quite helpful.
So, if you’re someone whose eyes start to roll at the thought of a continuum, I get it!
Roll your eyes and then consider why a Continuum of Trauma Care Matters.
A Continuum of Trauma Care helps trauma survivors make sense of and make the most of their experiences with different professionals, settings, organizations, and systems.
There are countless ways that trauma survivors interact with professionals, settings, organizations, and systems. Having a continuum to consider can really help them to:
- Place their experience. If they have a supportive experience, chances are the professionals, setting, organization, or system has some understanding and responsiveness regarding trauma. If the experience doesn’t feel good, or worse is triggering, then chances are understanding and responsiveness for trauma are low. Being able to see this along a continuum makes it less likely that the trauma survivor will blame themselves or accept being blamed for poor experiences.
- Access the right supports. Trauma survivors need the right supports. The continuum can help them filter out different possibilities, whether they are looking for the right school for their children or a community centre. It especially matters when it comes to finding supports. Trauma Care is like a lens that changes everything about how someone is seen, understood, assessed, communicated with, included, and treated. A trauma survivor that is dealing with someone who is “trauma unaware” will be frustrated and misunderstood. They are unlikely to come away with understanding, let alone the right diagnoses and referrals.
This is very important because many trauma survivors, especially when the trauma occurred in childhood, don’t know they are suffering from trauma. They are struggling with symptoms. They rely on practitioners to see the big picture and connect the dots that all of the symptoms are a reflection of underlying, unresolved trauma.
Further, different mental health practitioners land all across the continuum of trauma care. Sadly, some are trauma unaware, although this is becoming less common. Others might understand trauma and its impacts but are not specifically trained in how to facilitate recovery. Working with a therapist who is only trauma informed can protect against re-traumatization but may prolong recovery unnecessarily. And even those who are trauma trained have different levels of expertise. Some may be experienced with post traumatic stress disorder (level 1), but not complex trauma (level 2). As such, they will be able to support recovery for the overlapping symptoms of trauma, but will not have the expertise to recognize or work effectively with issues such as self-concept, insecure attachment styles, subconscious emotional learning, learned helplessness, somatic distress and symptoms, etc.
Then there is the question of responsibility. In our western society that places such a strong emphasis on the individual there is a risk that anyone, including mental health professionals will put an overemphasis on the survivor for struggling (victim blaming) and for recovering. On one hand, that is true. Only the survivor can take responsibility for their own recovery. But wrapped around that survivor, we need to hold the larger truth that the prevalence of trauma is a reflection of and toxic result of such things as long standing intergenerational family dysfunctions and a larger society with pervasive issues of colonialism, inequality and injustice, much of which results in trauma to the individual and to groups of individuals with lesser power and privilege.
A Continuum of Trauma Care Helps Drive Practice Change.
When things are laid out using a continuum, they actually take the complex and attempt to clarify it in one or more ways. This clarification helps to drive change because it lays things out so we can see the degrees of something. In this case, the degrees of trauma care.
This differentiation helps individuals, groups, settings, organizations, and systems to locate and identify themselves along the continuum. And it helps them know where to reach for, and hopefully motivates them toward improvement.
From what I know, at the onset of change, there wasn’t so much a continuum as there were two labels: trauma aware or trauma unaware (in reality it was more like trauma ignorant/victim blaming).
There are many different depictions. Some only have two levels, while others have three or four. It really depends on how many concepts the continuum is trying to clarify.
The one I developed is how I see it at the present time. In truth, I redid the visual about six times until it felt reflective and covered all of the concepts that I felt were relevant and important.
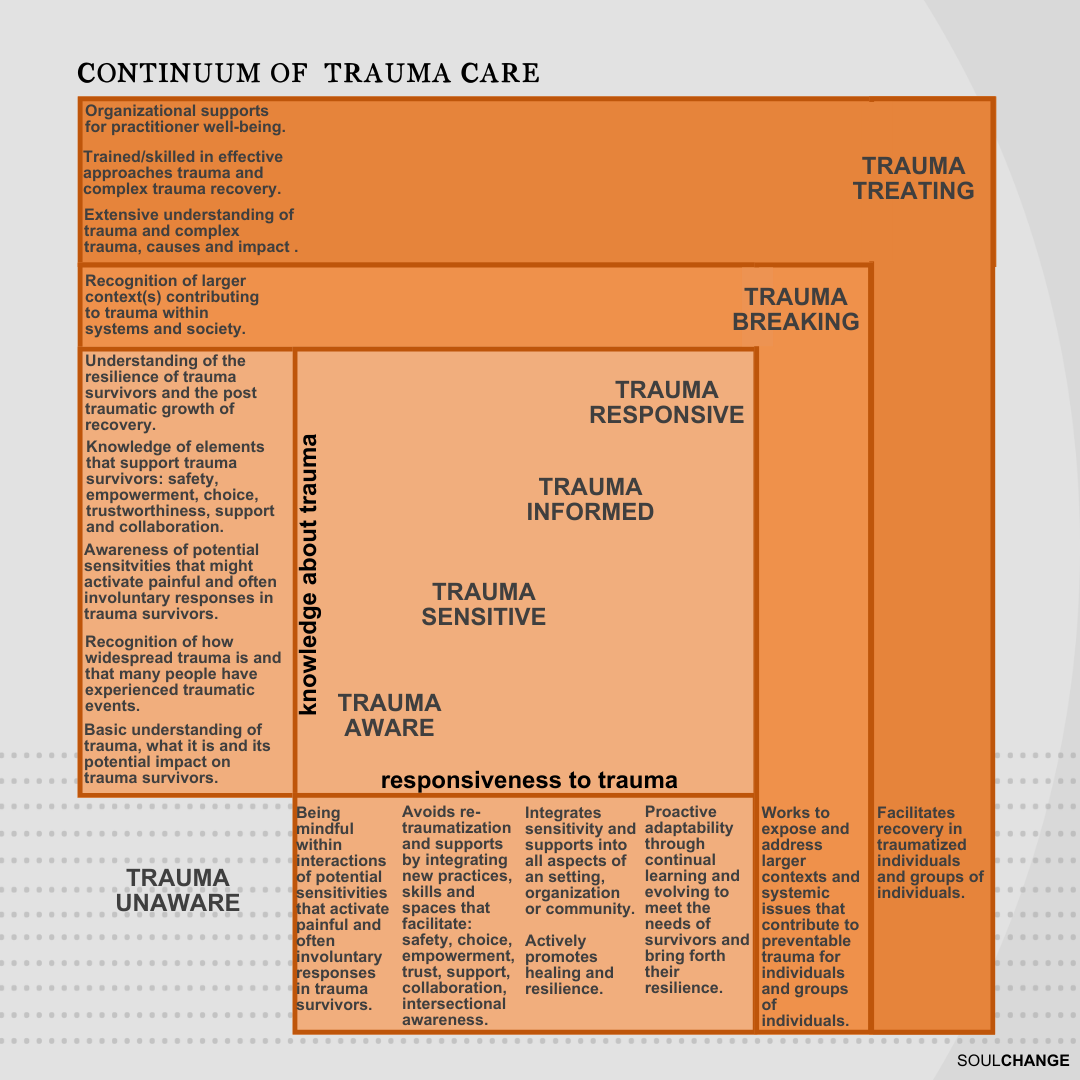
Let me dig in and explain the seven groupings a little, although I hope it’s pretty self-explanatory. I believe the groupings apply to individuals, groups, settings, organizations, communities, and systems, and reflect degrees of knowledge about trauma and responsiveness to trauma.
- Trauma Unaware– are those that have no to limited knowledge or responsiveness to trauma.
- Trauma Aware– are those that have a basic knowledge of trauma, as well as its prevalence, its impacts, and use a mindful response that demonstrates sensitivity for environments, circumstances, and interactions that might activate painful, often involuntary responses in trauma survivors.
- Trauma Sensitive– are those that move beyond basic knowledge of trauma and mindful responses that demonstrate sensitivity to providing environments, circumstances and interactions that actively avoid re-traumatization and offer supports by integrating new skills, practices, and spaces that facilitate safety, empowerment, choice, trust, support, collaboration, and awareness for intersectional issues (gender, cultural, historical, etc.)
- Trauma Informed- are those that further increase their understanding and responsiveness and integrate trauma sensitivity and supports into all aspects of and setting, organization, or community. They promote healing and resilience including through trauma screening and referrals. They also recognize the resilience of trauma survivors and the post traumatic growth that emerges though recovery.
- Trauma Responsive– are those that engage in continually adapting and learning to meet the needs of trauma survivors and bring forth their resilience, recovery, and post-traumatic growth. They do things like evaluating, incorporating emerging research, updating practices and policies, and seeking input from survivors.
- Trauma Breaking- are those that are trauma knowledgeable and responsive, who have gone further with their responsiveness in a way that exposes and tries to address the larger context, systems, and social issues that contribute to preventable trauma. They are the individuals and groups trying to make change related to such things as human rights, Truth and Reconciliation, the aspects of intersectionality, child abuse and neglect, family violence, psychologically unsafe work environments. They recognize these issues as perpetuating trauma and seek to have them resolved for the good of all.
- Trauma Treating- are those practitioners and organizations that have extensive knowledge and significant responsiveness to those living with trauma. They are additionally trained and support recovery of individuals with trauma. However, even within this level, there is a range of responsiveness among practitioners. Some are trained to support survivors in addressing post-traumatic stress disorder, and others have much more extensive training and experience and are equipped to support survivors of complex trauma.
Why Understanding a Continuum of Trauma Care Might Matter to You
All of this is well and good. There’s a Continuum of Trauma Care.
Assuming you haven’t disengaged, what’s really important is how it might matter for you.
If you’re a trauma survivor or someone close to you is (and it feels safe and comfortable to do so):
- Hold up the Continuum and look through it based on your/their experiences interacting with those in helping roles, settings, organizations, and systems. Did things trigger you? Did you feel terribly misunderstood? Were you blamed or told something was just in your head? Or were you helped to feel safe and make better sense of things?
- Consider the Continuum in terms of any trauma supports you have specifically sought or are planning on seeking. Are they “trauma treating” in terms of training and experience at the level, whether it is post trauma or complex trauma, you need to ensure you will not be re-traumatized or stuck in prolonged recovery?
If you’re a trauma survivor or someone close to you is and now is not the best time, then just tuck the Continuum of Trauma Care away for now. Pull it out when the time feels more right.
With Humility, Hope, and Heart,